Bariatric surgery has evolved significantly in recent years, offering patients safer procedures, faster recoveries and better long-term outcomes. Bariatric surgeons at the Metabolic & Weight Management Center in Pinehurst say new technologies, particularly robotic-assisted surgery, are transforming how weight-loss procedures are performed and how patients recover.
Below, bariatric surgeons with the Metabolic & Weight Management Center and Pinehurst Surgical Clinic David Grantham, M.D., and Raymond Washington, M.D., discuss the latest advances in bariatric surgery, the procedures offered today and what the future may hold for patients seeking treatment for obesity.
Q: What is new in bariatric surgery today—from robotics to revision procedures?
Dr. Grantham: Over the past couple of years, we’ve begun performing many of our bariatric procedures using robotic-assisted surgery. We’ve found that it has made a meaningful difference in patient recovery. Patients tend to feel better faster and are often ready to go home sooner than with traditional approaches.
Our outcomes have been excellent, and we’re consistently seeing the benefits for patients in terms of both recovery and overall results.
Q: What has changed the most in bariatric surgery, and what does it mean for patients?
Dr. Washington: Several things have changed in recent years. Medications such as GLP-1 drugs have certainly brought more public attention to weight loss. But there remains a group of patients who need surgical intervention—particularly those who may need to lose 100 pounds or more.
Advances in minimally invasive and robotic surgery have made these procedures much easier for patients to undergo. Many of our patients stay in the hospital only overnight, recover quickly and return to work in about two weeks.
Just as important, the complication rates are significantly lower than they were decades ago when bariatric surgery was performed as an open operation. Today, patients can achieve excellent outcomes while returning to normal activities much sooner.
Q: Bariatric surgery once had a reputation for long recoveries and major lifestyle adjustments. Is that still the case?
Dr. Washington: It’s very different today. Because we operate through small incisions, the risk of complications such as hernias or infections is much lower. Patients recover more quickly and are able to resume their daily routines sooner.
In fact, some studies have shown that bariatric surgery can be as safe—or even safer—than other common procedures, such as gallbladder removal. That’s an important message for patients who may still think of bariatric surgery the way it was performed 20 years ago.
Dr. Grantham: The difference is remarkable. We’ll often see patients the morning after surgery already dressed and asking when they can go home. Even five years ago that was less common. Compared to the days when these procedures were done through large open incisions, the progress has been tremendous.
Q: Robotic-assisted surgery is becoming more common across many specialties. How has robotics changed bariatric surgery specifically?
Dr. Grantham: The robotic platform allows the surgeon to use instruments that have wrist-like movement inside the body. That added dexterity makes it easier to perform delicate steps, such as sewing two sections of intestine together or connecting the stomach and small intestine during a gastric bypass.
Another advantage is the enhanced visualization. The robotic system provides a magnified, three-dimensional view of the anatomy, allowing surgeons to see structures with greater clarity.
For patients who are unfamiliar with the technology, it’s important to note that the surgeon is still performing the procedure. The robot is simply a tool that allows us to operate with greater precision and control.
Q: What bariatric procedures are offered at the Metabolic & Weight Management Center?
Dr. Washington: The two primary procedures we perform are sleeve gastrectomy and gastric bypass, both of which can be done laparoscopically or with robotic assistance.
A sleeve gastrectomy typically takes less than an hour to perform. During the procedure, about 80 percent of the stomach is removed, leaving a smaller, sleeve-shaped stomach. Because patients feel full more quickly, the procedure helps them lose about 50 to 70% of their excess body weight over the first 9 to 18 months. It’s considered a restrictive procedure because it limits how much food the stomach can hold.
The gastric bypass, long considered the gold standard in bariatric surgery, works in two ways. First, we create a smaller stomach pouch so patients eat less. Second, we reroute a portion of the small intestine, which reduces the number of calories absorbed.
Patients who undergo gastric bypass often lose slightly more weight—typically about 60 to 80 percent of their excess body weight. Like the sleeve procedure, gastric bypass is usually performed robotically, with most patients going home the next day and returning to work within about two weeks.
Q: What exactly is bariatric revision surgery, and how does it differ from a patient’s first procedure?
Dr. Grantham: Revision surgery refers to an operation performed on someone who has previously had bariatric surgery. In some cases, a patient’s anatomy may need to be modified to address symptoms or to improve weight-loss results.
One of the most common revision procedures we see today involves gastric bands. Gastric banding was widely performed years ago but is rarely done in the United States today. Many patients who previously had a band placed are now having it removed and converted to either a sleeve gastrectomy or a gastric bypass.
Another scenario involves patients who previously had a sleeve gastrectomy but later develop severe reflux. In those cases, converting the sleeve to a gastric bypass can often provide better reflux control while continuing to support weight loss.
Q: What are some of the most common reasons patients might consider revision surgery?
Dr. Washington: There are a few primary reasons. As Dr. Grantham mentioned, severe reflux is one of them. Gastric bypass has long been known to significantly reduce heartburn symptoms, so patients experiencing reflux after a sleeve procedure may benefit from conversion to a bypass.
Other reasons may include inadequate weight loss or complications related to earlier procedures that are no longer commonly performed. Revision surgery allows us to correct those issues and provide patients with a more effective, modern approach to bariatric treatment.
Q: Looking ahead, what excites you most about the future of bariatric surgery?
Dr. Grantham: The future is very broad and exciting. While surgery will continue to play an important role, treatment may increasingly involve a combination of therapies. These could include endoscopic procedures, medications and surgical options working together to achieve the best outcomes for patients.
As surgeons, we’re uniquely positioned to offer all of those tools. Whether it’s performing an operation, conducting an endoscopic procedure or prescribing medication, our goal is always to find the safest and most effective solution for each individual patient.
Dr. Washington: I’m also excited about how much focus there is now on long-term success. In our program, surgery is just one part of the journey. We use a multidisciplinary approach that includes nutrition specialists, behavioral health support and ongoing follow-up care.
We see patients at regular intervals after surgery—three months, six months, nine months and one year—but in many ways we consider them part of our program for life. That long-term partnership helps patients maintain their weight loss and continue building healthier habits.
Ultimately, our goal isn’t just to help patients lose weight—it’s to support them in achieving lifelong health.
To learn more about weight-loss surgery at the Metabolic & Weight Management Center in Pinehurst, N.C., visit www.WeightLossNC.org.







A family affair: Along with a full staff, Owner Eddie Claude and his wife Ruth (pictured right) work with their kids to run the restaurant. Eddie is a Veteran who served for 21 years in the U.S. Army. Photos by YGH STUDIOS & GFBJ. The Fayett
With summer in full swing, I started to reflect on the various ways I spent my summer break over the years. From pool parties with friends to family vacations and sports tournaments, I look back fondly on the summers I’ve enjoyed so far. But it
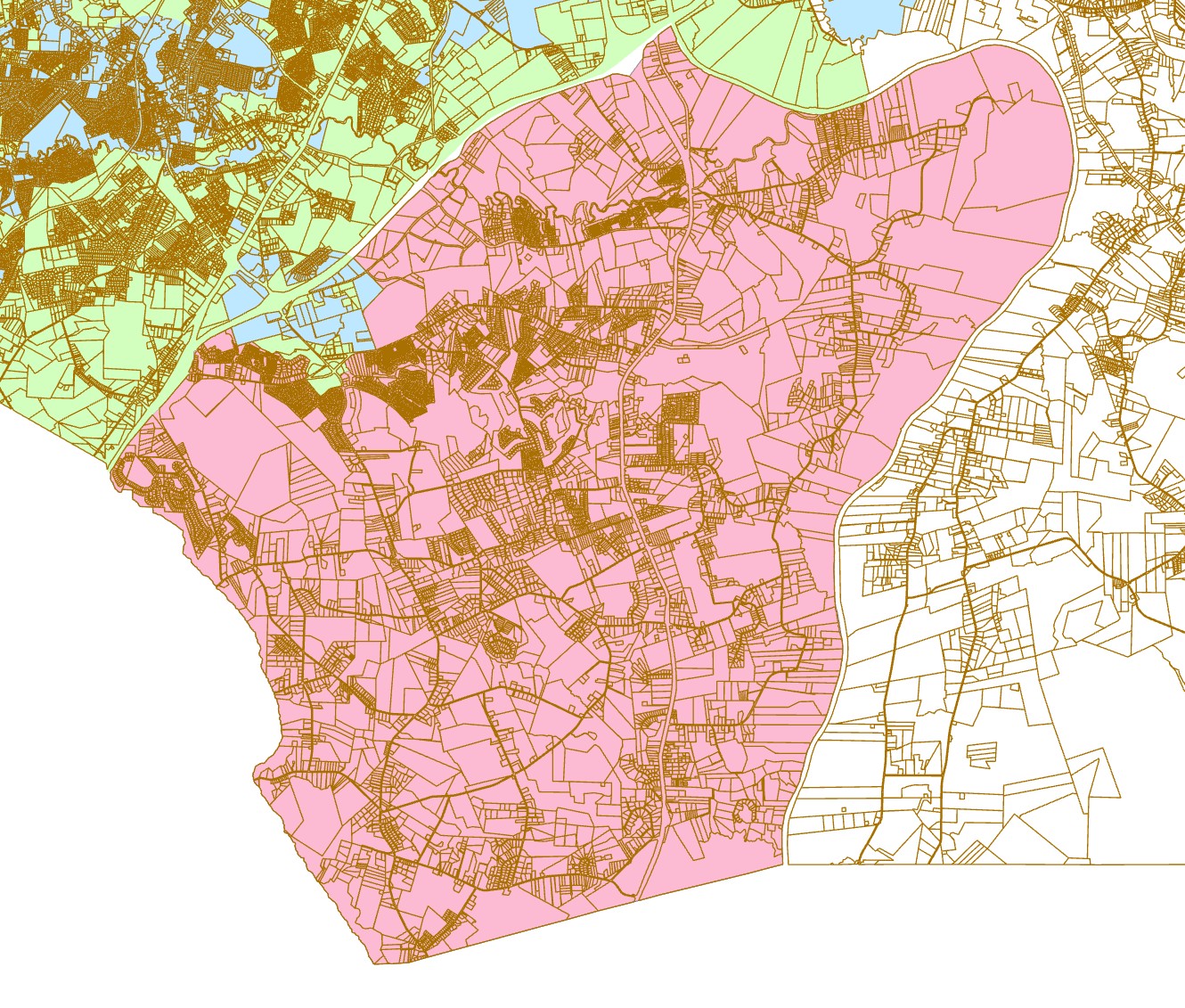
Proposed incorporation boundary (pink) · Gray’s Creek, Cumberland County, N.C. This is a working draft and is subject to revision. Image courtesy of grayscreeknc.com. After decades as an unincorporated rural community in Cumberland County, Gray’